Once, I was bitten by the Neurosurgery bug. (Thanks, Dr. Ojemann!) Before I became a radiologist, I researched vasospasm in Sub-arachnoid Hemorrage (SAH). It was a fascinating problem, unfortunately with very real effects for those afflicted. Nimodipene and the old “triple-H” therapy were treatment mainstays. Many Neurosurgeons added their own ‘special sauce’ – the treatment du jour. For In Vitro (in the lab) experimental interventions held great promise for this terrible complication, but nearly all would fail when applied in clinical practice, In Vivo (in real life).
As physicians, we look at disease and try to find a “silver bullet” which will treat that disease 100% of the time with complete efficacy and no side effects. Using Occam’s Razor, the simplest & most obvious solution is often the best.
Consider a disease cured by a drug, as in figure 1. Give the drug, get the desired response. The drug functions as a key in the lock, opening up the door.

This is how most carefully designed In Vitro experiments work. But take the treatment out of the laboratory, and it fails. Why?
The carefully controlled lab environment is just that – controlled. You set up a simple process, and get your result. However, the In Vivo environment is not so simple – competing complex processes maintaining physiologic homeostasis, at the cellular bio-chemical level – interact with your experiment & confound the results. And the number of disease processes that involve a simple direct cure dwindle with time – the previous generations of scientists have culled those low-hanging fruit already! You are left with this:
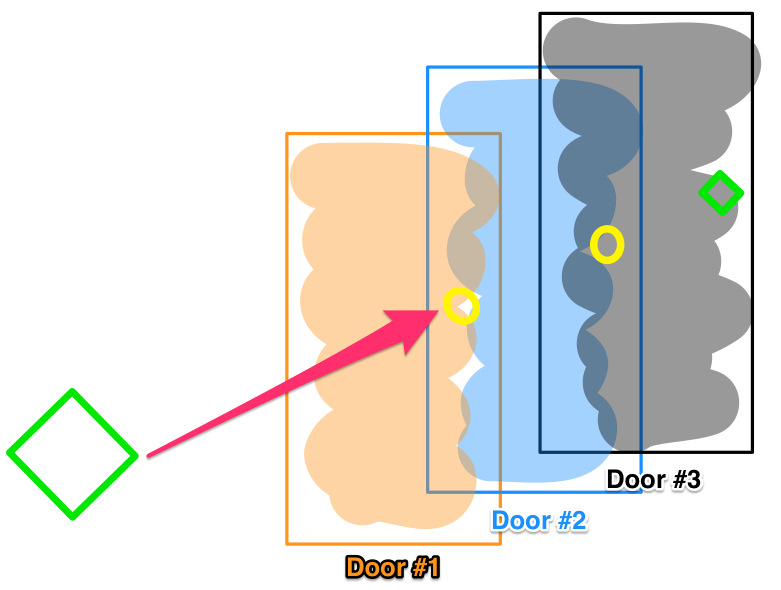
Consider three locked doors, one after the other. You can’t open the second without opening the first, and you can’t open the third without opening up the first and second. Here, we have a good therapy, which will cure the disease process , represented by opening up door #3. But the therapy cannot get to Door #3 – it’s blocked by Doors #1 and #2.
Considering the second system, which more closely approximates what we find in real life, an effecacious drug or treatment exists, which can’t get to the disease-impacting pathway, because it is “locked out” by the body’s other systems. Not exhaustively: Drug elimination, enzymatic drug inactivation, or feedback pathways counteracting the drug’s effec – it works, but the body’s own homeostatic mechanisms compensate!
Experimentally though, we are not taught to think of this possibility – instead preferring a single agent with identifiable treatment results. However, many of these easy one-item solutions have already been discovered. That’s why there has been a decrease in the number of novel synthetic chemical drug discoveries lately, as opposed to growth in biologics. Remember monthly new antibiotic releases? How often do you see new antibiotics now?
There is a tremendous opportunity to go back and revisit compounds that have been initially discarded for reasons other than toxicity to see if there are new or synergistic effects when combined with other therapy. Randomized controlled trials would be too large and costly to perform a priori on such compounds – but using EHR data mining, cross-validated longitudinal trials could be designed from existing patient data sets, and some of these unexpected effects could be elucidated after the fact! Then a smaller, but focused, prospective study could be used to confirm the suspected hypothesis. Big data analytics has great promise in teasing out these relationships, and the same techniques can be applied to non-pharmacologic interventions and decisions in patient care throughout medicine. In fact, the answers may already be there – we just may not have recognized it!
P.S. Glad to be back after a long hiatus. Life happens!