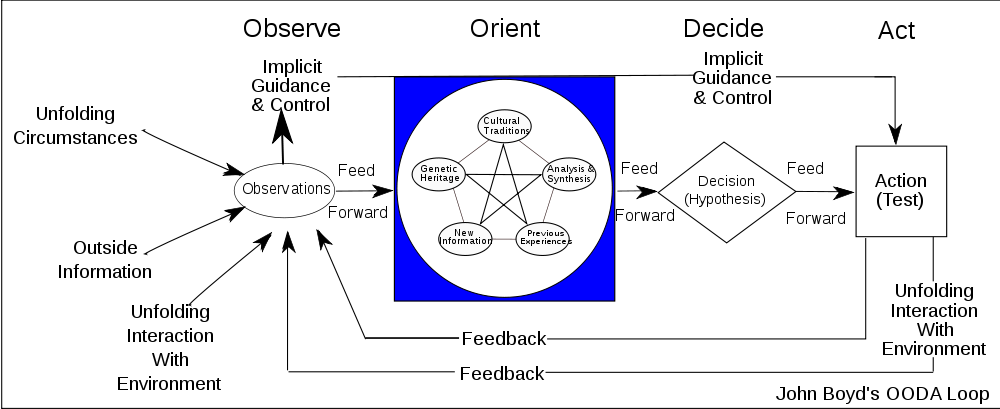
John Boyd was a US military pilot who became a military strategist. His chief contribution to military theory was contained in a large slide presentation and one essay, but his teachings heavily influenced those who train our military commanders and are incorporated into US military strategy and tactics. Boyd characterized the decision-making process as a means of a continuous (iterative) cycle of Observation – Orientation – Decision – and Action. This OODA loop is the mechanism enabling adaption and therefore survival.
The observation process involves data gathering, orientation is analysis and synthesis, decision is determination of course of action, and action is the execution of that decision, with resultant consequence. Boyd felt that any model is incomplete (including our own perception of reality) and must be continuously refined or adapted in the setting of new data. This is in the setting of increasing entropy (disorder, uncertainty) of any system once it perturbs from the initial point, which we perceive incompletely and imprecisely due to our human limitations. There’s actually a not insubstantial amount of philosophic thought in that!
It is easiest to conceive of the OODA loop in the setting of a dogfight between two fighter pilots. Each pilot is feeling out the other, maneuvering in a certain way that will best give them the kill, ensuring their own personal survival. The OODA loop is by definition, reactive. But the victorious pilot will be able to out-think his opponent by leaving his own OODA loop and getting inside his opponent’s OODA loop, and therefore predict what that pilot is likely to do. That ability to be predictive with a reasonable certainty, allows the winning pilot to best his opponent, all other things being similar. (skill, plane, etc..)
OODA loops have been applied successfully in business, sports, and particularly in litigation.
In healthcare, physicians have their own worldview or OODA loop. They observe patients, orient their differential, decide on a diagnosis and treatment, and then act on that treatment and observe their results, trying something else if unsuccessful. More experienced or better clinicians have very well-developed, almost algorithmic, OODA loops. They also are functioning in their environment (the practice, the wards, the OR) where they have very specific, well-developed skills to assess when something is amiss – patient flow, quietness, absence of something as opposed to glaring signs (like alarms, etc…).
You could hardly expect the healthcare administrator to have the same OODA loop. Note the Cultural Traditions in the blue box – very different for both! So when the two interact, so do these loops, and may lead to some unsatisfying conversations if there is no empathy between the administrator and the physician. The physician communicates to the administrator, and the administrator communicates back, but neither is understanding what the other is saying. It probably falls upon the more emotionally intelligent of the two to try to get inside the OODA loop of the other to facilitate a truly constructive conversation. Without practiced understanding, the physician risks being labeled ‘disruptive’ and the administrator risks being thought of as ‘unfair’.
Venkatesh Rao, of the sublime ribbonfarm blog, has an older post on his Tempo book blog about OODA’s backstory. I have ‘borrowed’ his OODA diagram here.
I finally got around to writing the companion update to this post – it concerns OODA loops and AI. I invite you to read it.