Consider an adult patient who has presented to the ER for abdominal pain. The ER doctor suspects an appendicitis, so next is a CT scan to “r/o appendicitis.” There is an assumption that the patient has already had labs drawn and done upon presentation to the ER (probably a rapid test).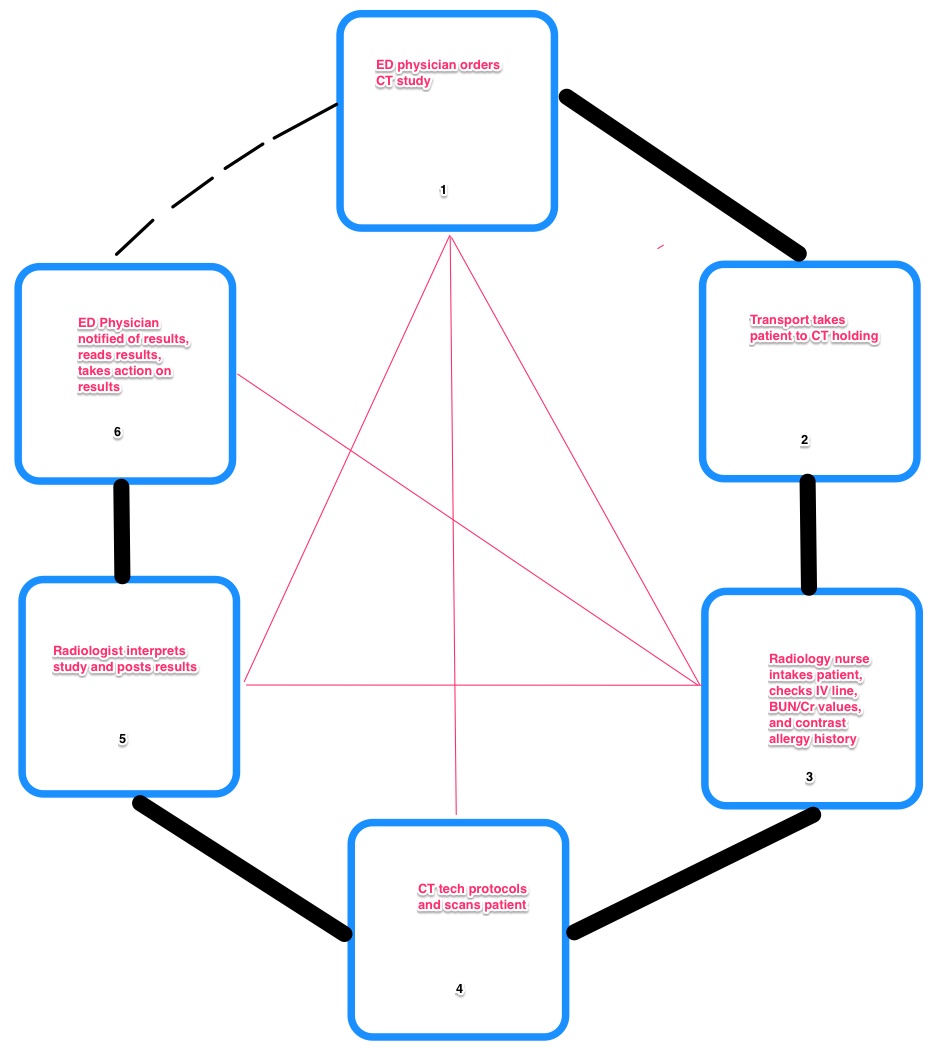
First, the ER doctor has to decide to order the CT study, and write the order. We’ll assume a modern CPOE system to take out the intervening steps of having the nurse pick up the order, sign off, and then give it to the HUC to call the order to the CT technologist. We’ll also assume that the CPOE system automatically contacts patient transport and lets them know that there is a patient ready for transport. Depending on your institution’s HIMSS level, these may be a lot of assumptions!
Second, patient transport needs to pick up the patient and bring them to the CT holding area (from the hallway to a dedicated room).
Third, the nurse (or a second technologist / tech assistant) will assess this patient and make sure that they are a proper candidate for the procedure. This involves taking a focused history, making sure there is no renal compromise that would be made worse by the low osmolar contrast (LOCA) used in a CT scan, ensuring that IV access is satisfactory for the LOCA injection (or establishing it if it is not), and ensuring that the patient does not have a contrast allergy that would be a contraindication to the study.
Fourth, the CT technologist gets the patient from holding, places them on the CT gantry, hooks up the contrast, and protocols the patient, and then scans. Once the scan finishes, the patient returns to holding, and the study posts to the PACS system for interpretation by the M.D. radiologist.
Fifth, the radiologist physician sees the study pop up on their PACS (picture archiving & communication system), interprets the study, generates a report (usually by dictating into voice recognition software these days), proofreads it and then approves the report. If there is an urgent communication issue, the radiologist will personally telephone the ER physician, if not, ancillary staff on both sides usually notice the report is completed and alerts the ER physician to review it when he has time.
Sixth, the ER physician sees the radiologist’s report. She or he then takes all the information on the patient, including that report, laboratory values, physical examination, patient history, and outside medical records and synthesizes that information to make a most likely diagnosis and exclude other diagnoses. It is entirely possible that the patient may go on to additional imaging, and the process can repeat.
In comparison to the prior model where all interactions were considered, we can use a bit of common sense to get the number of interacting terms down. The main rate limiting step is the ordering ER physician – the process initiates with that physician’s decision to get CT imaging. It is possible for that person to exceed capacity. Also, there are unexpected events which may require immediate discussion and interaction between members of the team – ER physician to either radiology physician, radiology nurse, or radiology technologist. Note that the radiology physician and the radiology nurse can both interact with the ER physician both before (step 1) and after (step 6) the study, because of the nature of patient care.
An astute observer may note that there is no transport component of the patient back to ER from radiology holding. This is because the patient has already been assessed by the ER physician, and more testing, disposition, etc… is pending the information generated by the CT scan. While the patient certainly needs care, where that care is given during the assessment process (for a stable patient )is not critical. It could be that the patient goes from CT holding to dialysis, or another testing area, etc… Usually the next ordered test, consult, or disposition hinges on the basis of the CT results, and will be entered via CPOE, where the patient and ER physician need not be in the same physical space to execute.
From practical experience, ER physician – CT technologist interactions are most common and usually one-sided. (please take this patient first, I want the study done this way, etc…) ER physician – nurse interactions are uncommon and usually unidirectional (nurse to physician – this patient is in renal failure, we can’t use LOCA, etc…). ER Physician and radiology physician interactions are even less common but bidirectional. (‘This patient is confounding – how can we figure this out?’ vs. ‘your patient has a ruptured aortic aneurysm and will die immediately without surgical interaction!’)
Next post we will modify our generalized linear model and begin assembling a dataset to test our assumptions.