
For a new definition of value, it’s helpful to go back to the conceptual basis of payment for medical professional services under the RBRVS. Payment for physician services is divided into three components: Physician work, practice expense, and a risk component.
Replace physician with provider, and then extrapolate to larger entities.
Currently, payer (insurer, CMS, etc…) and best practice (specialty societies, associations like HFMA, ancillary staff associations) guidelines exist. This has reduced some variation among providers, and there is an active interest to continue this direction. For example, level 1 E&M clearly differs from a level 5 E&M – one might disagree whether a visit is a level 3 or 4, but you shouldn’t see the level 1 upcoded to 5. Physician work is generally quantifiable in either patients seen or procedures done, and for any corporate/employed practice, most physicians will be working towards the level of productivity they have contractually agreed to, or they will be let go/contracts renegotiated. Let’s hope they are fairly compensated for their efforts and not subjected solely to RVU production targets, which are falling out of favor vs. more sophisticated models (c.f. Craig Pedersen, Insight Health Partners).
Unless there is mismanagement in this category, provider work is usually controllable, measurable, and with some variation due to provider skill, age, and practice goals, consistent. For those physicians who have been vertically integrated, their current EHR burdens and compliance directives may place a cap on productivity.
Practice expenses represent those fixed expenses and variable expenses in healthcare – rent, taxes, facility maintenance, and consumables (medical supplies, pharmaceuticals, and medical devices). Most are fairly straightforward from an accounting standpoint. Medical supplies, pharmaceuticals, and devices are expenses that need management, with room for opportunity. ACO and super ACO/CIO organizations and purchasing consortiums such as Novation, Amerinet, and and Premier have been formed to help manage these costs.
Practice expense costs are identifiable, and once identified, controllable. Initially, six sigma management tools work well here. For all but the most peripheral, this has happened/is happening, and there are no magic bullets out there beyond continued monitoring of systems & processes as they evolve over time as drift and ripple effects may impact previously optimized areas.
This leaves the last variable – risk. Risk was thought of as a proxy for malpractice/legal costs. However, in the new world of variable payments, there is not only downside risk in this category, but the pleasant possibility of upside risk.
It reasons that if your provider costs are reasonably fixed, and practice expenses are as fixed as you can get them at the moment, that you should look to the risk category as an opportunity for profit.
As a Wall St. options trader, the only variable that really mattered to me for the price of the derivative product was the volatility of the option – the measure of its inherent risk. We profited by selling options (effectively, insurance) when that implied volatility was higher than the actual market volatility, or buying them when it was too low. Why can’t we do the same in healthcare?
What is value in this context? The profit or loss arising from the assumption and management of risk. Therefore, the management of risk in a value-based care setting allows for the possibility of a disproportionate financial return.
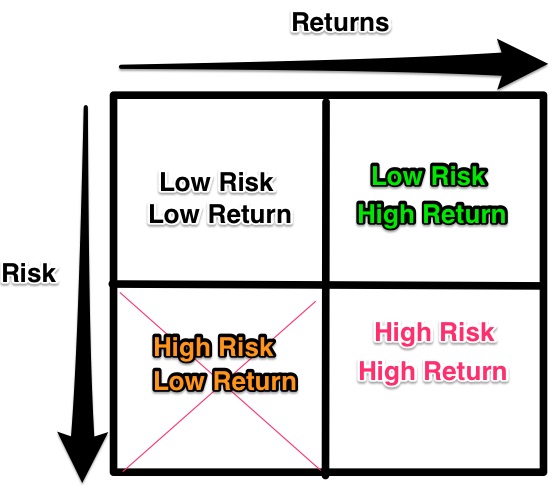
- Low risk/low return – not worth your time.
- High risk/low return – stay as conservative as possible (think robust systems and processes).
- High Risk/High return can be titillating & terrifying at the same time, just have open eyes and realistic expectations about what you are doing and possible outcomes, including the demise of your institution & career(!)
The sweet spot is Low Risk/High Return. This is where discovering a fundamental mispricing can return disproportionately vs. exposure to risk.
Apply this risk matrix to:
- 1 – A medium sized insurer, struggling with hospital mergers and former large employers bypassing the insurer directly and contracting with the hospitals.
- 2 – A larger integrated hospital system with at-risk payments/ACO model, employed physicians, and local competitors which is struggling to provide good care in the low margin environment.
- 3 – group radiology practice which contracts with a hospital system and a few outpatient providers.
& things get interesting. On to the next post!