There is a maxim in management circles to use data-rich methods of management. Peter Drucker is reputed to have said, “What gets measured gets managed.” Clearly better than managing by the hem of one’s skirt (or seat of one’s pants), data-driven management allows for assessment of measured items.
It is interesting to consider the perturbations of this statement:
-if it can be measured, it can be managed (implying causality)
-if it can’t be measured, it can’t be managed (negative causality)
-if it can’t be measured, it doesn’t matter (reductio ad absurbum)
You can pick for yourself where in the spectrum you lie, and how far from Drucker’s original statement you are.
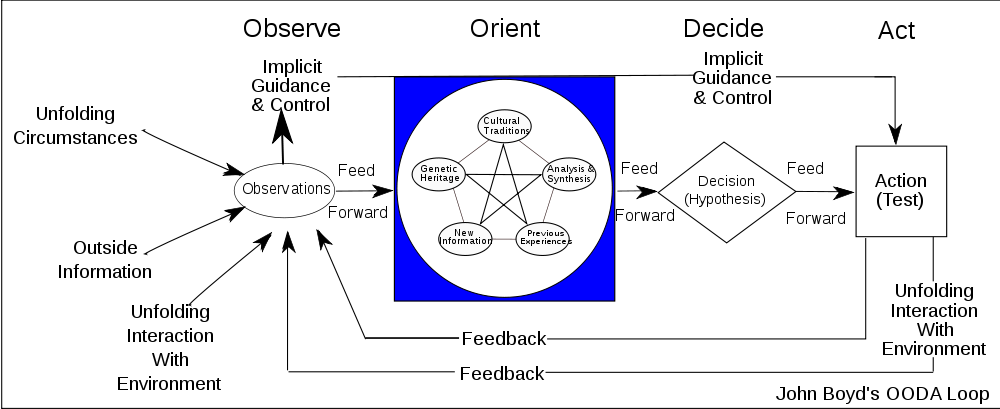
But there is another issue in measurement that isn’t as well addressed – the influence that the measure itself has on what is being measured. This is what is known as an observer effect in Physics – simply measuring perturbs the system. The Heisenberg uncertainty principal has been cited like this (that’s actually NOT what the Heisenberg says, but that’s beyond the scope of this discussion).
So, let’s acknowledge that observation, or measurement changes what is being measured itself. An observation, or ‘measure’ of X (insert variable here – productivity, speed, outcome, etc..) is performed. It is compared to a standard, or ‘metric’ is performed.
For a process or an person, there may or may not be established standards of measurement. Therefore, a baseline or initial measurement becomes the metric to compare future measurements against. As process improvement or skill improvement happens (hopefully), subsequent metrics should improve in both accuracy and value.
Let’s consider a human measure and its associated metric. A manager may wish to evaluate his employees by comparing their productivity to an established range of productivity. The employee is being measured, and is being compared to a metric.
But employees aren’t stupid. Even if they have not been told that they are being measured, when they see the difference in their performance reviews as compared to their peer’s performance reviews, they figure it out. And those employees with performance reviews that didn’t sit right with them become more diligent in their work, to achieve a better performance review next time. Some employees will even figure out that they are being evaluated, and up their game before the performance review.
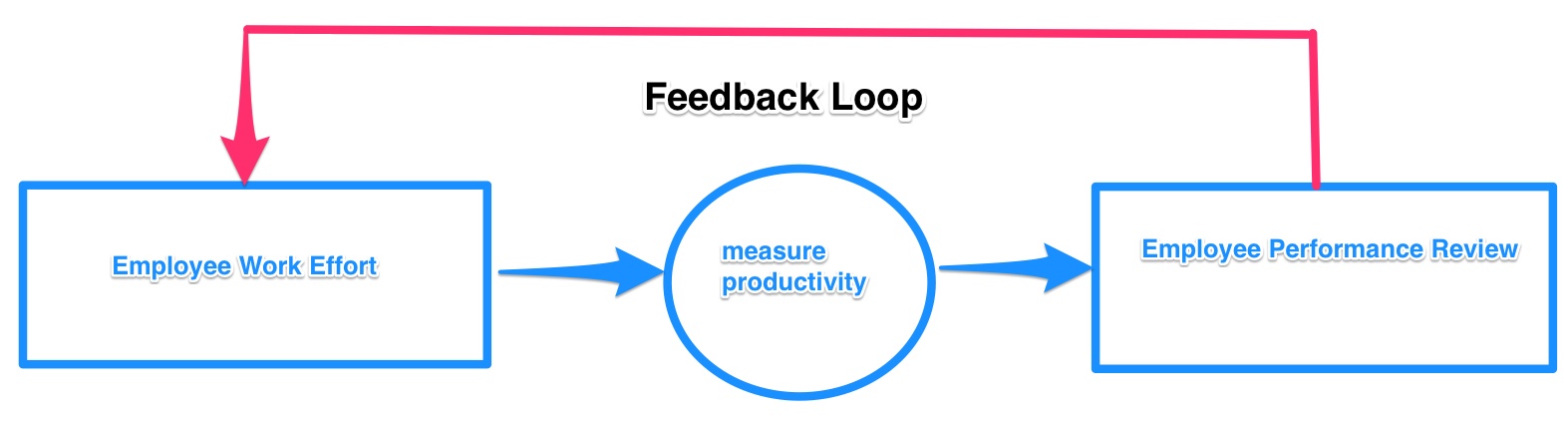
So, by the mere act of being measured, we change what is being measured. The measure is the metric.
And it shouldn’t be too hard to figure out that WHAT you measure and WHAT you choose to be the metric are more important than you think.