Systems trading on Wall Street in the early days (pre 1980’s) was done by hand or by laborious computation. Systems traded off indicators – hundreds of indicators, exist but most are either trend or anti-trend. Trending indicators range from the ubiquitous and time-honored Moving Average, to the MACD, etc… Anti-trend indicators tend to be based on oscillators such as relative strength (RSI), etc. In a trending market, the moving average will do well, but it will get chopped around in a non-trending market with frequent wrong trades. The oscillator solves some of this problem, but in a strongly trending market, tends to underperform and miss the trend. Many combinations of trend and anti-trend systems were tried with little success to develop a consistent model that could handle changing market conditions from trend to anti-trend (consolidation) and back.
The shift towards statistical models in the 2000’s (see Evidence-Based Technical Analysis by Aronson) provided a different way to analyze the markets with some elements of both systems. While I would argue that mean reversion has components of an anti-trend system, I’m sure I could find someone to disagree with me. The salient point is that it is a third method of evaluation which is neither purely trend or anti-trend.
Finally, the machine learning algorithms that have recently become popular give a fourth method of evaluating the markets. This method is neither trend, anti-trend, or purely statistical (in the traditional sense), so it provides additional information and diversification.
Combining these models through ensembling might have some very interesting results. (It also might create a severely overfitted model if not done right).
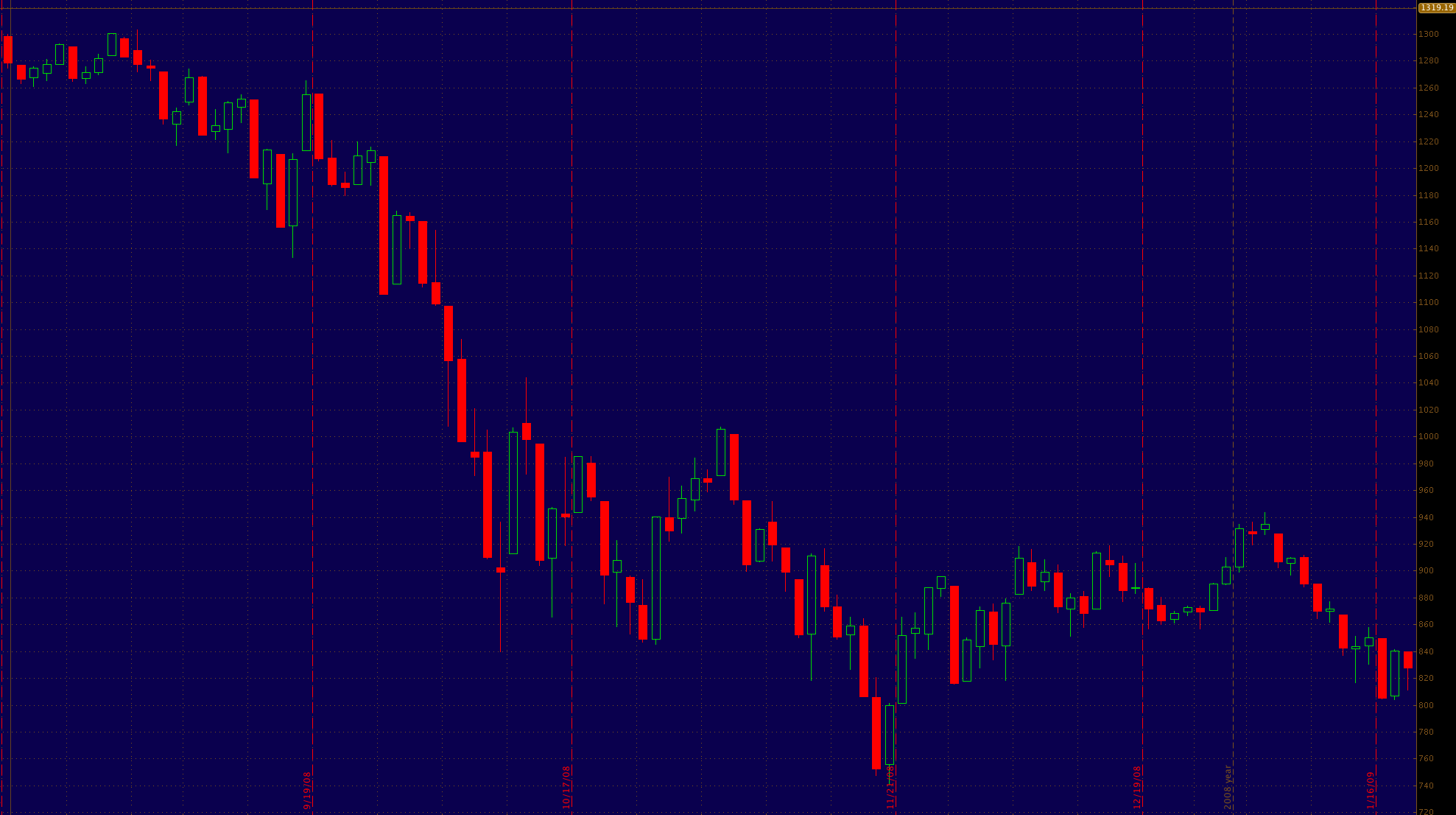
Sidebar: I believe that the market trades in different ways at different times. It changes from a technical market, where predictive price indicators are accurate, to a fundamental market, driven by economic data and conditions, to a psychologic market, where ‘random’ current events and investor sentiment are the most important aspects. Trending systems tend to work well in fundamental markets, anti-trend systems work well in technical or psychologic markets, statistical (mean reversion) systems tend to work well in technical or fundamental markets, and I suspect machine learning might be the key to cracking the psychologic market. What is an example of a psychologic market? This – the S&P 500 in the fall of 2008 when the financial crisis hit its peak and we were all wondering if capitalism would survive.
40% Drop in the S&P 500 from August – November during the 2008 financial crisis.
By the way, this is why you pay a human to manage your money, instead of just turning it over to a computer. At least for now.
So why am I bringing this up? I’m delving more deeply into Queuing & operations theory these days, wondering if it would be helpful in developing an ensemble model – part supervised learning(statistics), part unsupervised (machine) learning, part Queue Theory algorithms. Because of this, I’m putting this project on hold. But it did make me think about the algorithms involved, and I had an aha! moment that is probably nothing new to Industrial Engineering types or Operations folks who are also coders.
Algorithms, like an ensemble model composed of three separate models: a linear model (Supervised Learning), a machine learning model (Unsupervised learning) and a rule based models (Queueing theory), are software coded rule sets. However, the systems we put in place in physical space are really just the same thing. The policies, procedures and operational rule sets that exist in our workplace (e.g. the hospital) are hard-coded algorithms made up of flesh and blood, equipment and architecture, operating in an analogue of computer memory – the wards and departments of the hospital.
If we only optimize for one value (profit, throughput, quality of care, whatever), we may miss the opportunity to create a more robust and stable model. What if we ensembled our workspaces to optimize for all parameters?
The physical systems we have in place, which stem from policies, procedures, management decisions, workspace & workflow design, are a real-life representation of a complex algorithm we have created, or more accurately has grown largely organically, to serve the function of delivering care in the hospital setting.
What if we looked at this system as such and then created an ensemble model to fulfill the triple (quad) aim?